Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1 – Rationale and perspectives
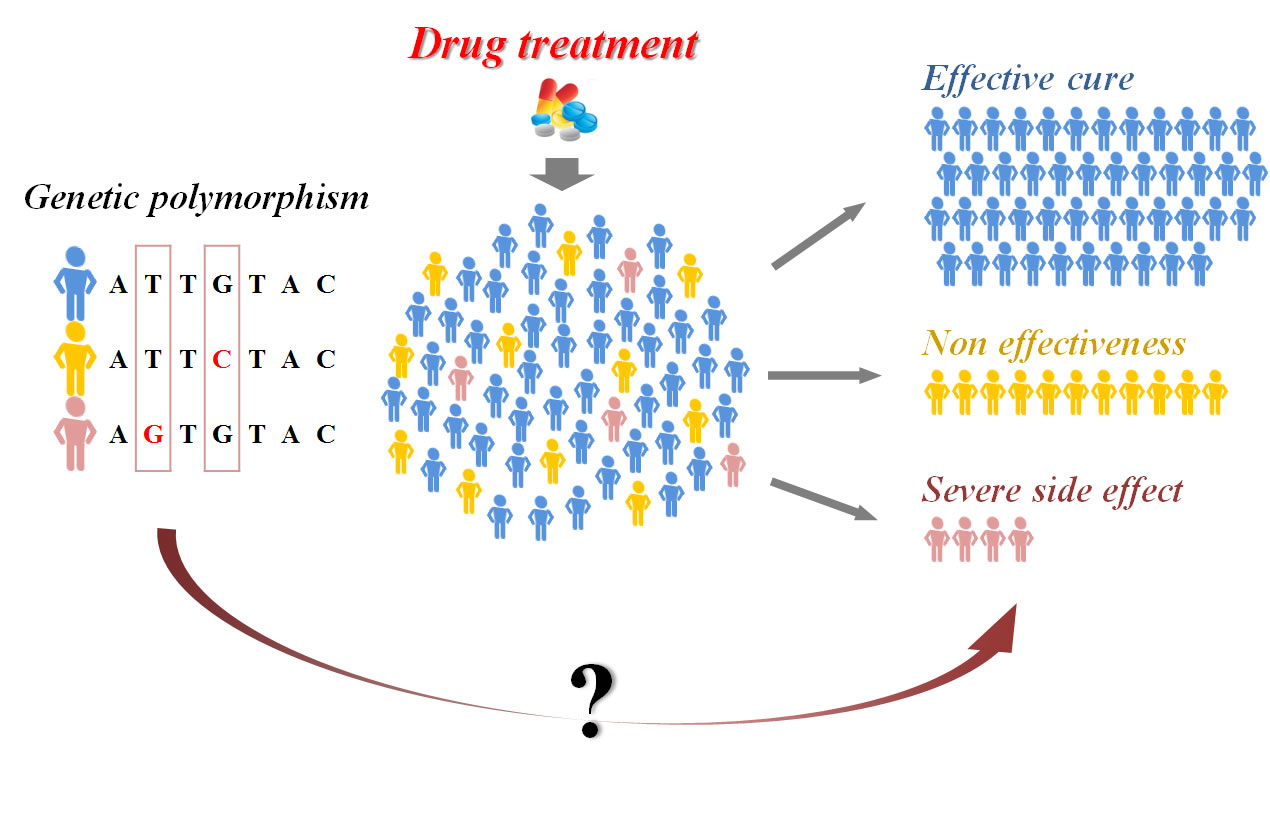
Warfarin is extensively prescribed as an oral anticoagulant for the prevention and treatment of thrombosis diseases. “An insufficient dose may fail to prevent thromboembolism, while an overdose increases the risk of bleeding” (Yin 2). The main genes looked at concerning the effect of warafin dosage are the CYP2C9 and VKORC1 genes.
Warfarin inhibited the vitamin K epoxide reductase (VKOR) which is encoded by the vitamin K epoxide reductase complex subunit 1 (VKORC1) gene. Demonstrated in Figure 1, Warfarin prevents the VKORC1 to regenerate reduced vitamin K from it’s epoxide form. The reduced version of vitamin K is needed as a cofactor for GGCX, an enzyme that catalyzes vitamin-K dependent clotting factors; thus having reduced coagulation. “Congential deficiencies in GGCX and VKORC1 have disordered hemostasis,” and “functional abnormalities in VKORC1…” are also Warfarin resistant (Yin 3).

Polymorphisms in CYP2C9
The functional sequences of the human CYP2C9 gene are the CYP2C9*1, the wild-type, and CYP2C9*2 and CYP2C9*3. Analysis showed patients with either “CYP2C9*2 or CYP2C9*2 variant require lower warfarin maintenance dose” (Yin 4). The risk for bleeding doubled in these patients, as they metabolize warfarin slower than the wild-type patient.
S-warfarin and R-warfarin make up the mixture of warfarin. “S-warfarin is a five-fold more potent vitamin K antagonist than R-warfarin…, metabolized primarily by CYP2C9”; this is also shown in Figure 1 (Yin 4).

Table 1 corresponds to the missense mutations mapped on Figure 2.

The table I have constructed below, Table 1.A, shows the variations of CYP2C9 alleles in varying ethnicities. This can give medical doctors a clue on how to better dose patients.

Polymorphisms in VKORC1
The two most commonly looked at polymorphism a inVKORC1 are the “1173C>T in intron 1 and 3730G>A in the 3′ untranslated region.” (Yin 5). The dosage for warfarin was higher in individuals with the VKORC1 1173CC variantion than those with the CT or TT variation. Patients with the 1173CT genotype have a higher risk from bleeding events was shown in a study of 330 patients.
Haplotypes analysis was carried out by constructing 5 haplotypes groups from the 10 most common SNPs, and their relationships to warfarin dose were examined in Caucasians. The table I have constructed, Table 2.A, below can explain “a large degree of the interindividual variations of a warfarin dose” (Yin 5).

Table 3 demonstrates the effects of VKORC1 alleles and haplotypes in varying ethnicities.

Other studies looking at the VKORC1 and CYP2C9 genes support the findings from above “that Asians require a lower average maintenance warfarin dose and African-Americans a higher average dose” (Yin 6).
Algorithms for warfarin dose determination
A dosing algorithm was created based on 297 Caucasian warfarin-treated patients, accounting for 55% of warfarin dose variability.
Dose=(0.628)-(0.0135)*(age, year)-0.240(CYP2C9*2)-0.370(CYP2C9*3)-0.241(VKORC1, -1639G>A)+0.0162*(height, cm)
For patients with homozygous wild-type for CYP2C9 and VKORC1 is below. Those with heterozygous or homozygous for CYP2C9, “the maintenance dose was further reduced by 1.3 and 2.9 mg respectively” (Yin 7).
(mg)=6.6-0.035*(age, year)+0.031*(body weight, kg)
Other alternative warfarin doses were developed by classifying patients into three groups called the “warfarin-response index”.
Perspective
Together the variations between CYP2C9, VKORC1, and “factors such as age, gender, body weight, height..”, and others can predict more than 33% of the variability in warfarin dosage. Ethnicity is an especially important factor too for doctors to use in prescribing warfarin (Yin 5). The author’s of this paper go on to say that genotyping in patients may not necessarily be cost-effective. “Treatment algorithms incorporating pharmacogenomic data must be evaluated prospectively in a randomized controlled clinical trial before incorporating into routine clinical practice” (Yin 8).
References
Yin, T. & Miyata, T. (2006). Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1 – Rationale and perspectives. Thrombosis Research, 120, 1-10. doi:10.1016/j.thromres.2006.10.021